{kind=link}

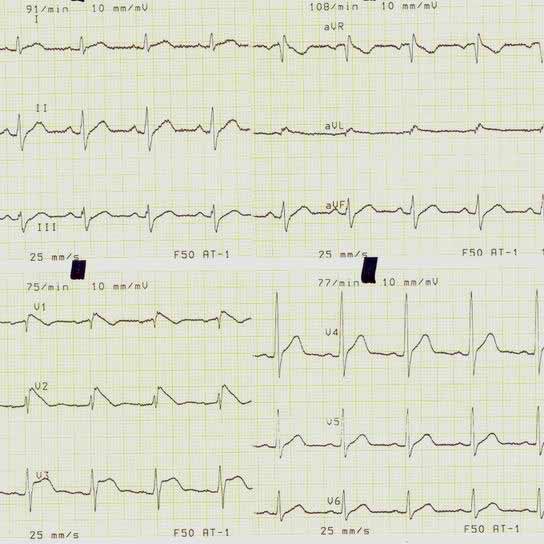
Three types of ST-segment elevation in Brugada syndrome, as shown in the precordial leads on ECG in the same patient at different times. Left panel shows a type 1 ECG pattern with pronounced elevation of the J point (arrow), a coved-type ST segment, and an inverted T wave in V1 and V2. The middle panel illustrates a type 2 pattern with a saddleback ST-segment elevated by >1 mm. The right panel shows a type 3 pattern in which the ST segment is elevated <1>
Pathophysiology
Accessory pathways or connections between the atrium and ventricle are the result of anomalous embryonic
 development of myocardial tissue bridging the fibrous tissues that separate the two chambers. This allows for electrical conduction between the atria and ventricles at sites other than the atrioventricular node (AVN). Passage through accessory pathways circumvents the usual conduction delay between the atria and ventricles, which normally occurs at the AVN and predisposes the patient to develop tachydysrhythmias.
development of myocardial tissue bridging the fibrous tissues that separate the two chambers. This allows for electrical conduction between the atria and ventricles at sites other than the atrioventricular node (AVN). Passage through accessory pathways circumvents the usual conduction delay between the atria and ventricles, which normally occurs at the AVN and predisposes the patient to develop tachydysrhythmias.
Lown-Ganong-Levine症候群
Pathophysiology
The syndrome described by Lown, Ganong, and Levine in 1952 associated the occurrence of tachycardia with presence of a short PR interval and normal QRS. Subsequent investigations have failed to identify a unifying anatomic basis that accounts for both occurrence of tachycardia and presence of a short PR interval. Rather, several mechanisms have been proposed for the coexistence of a short PR interval and normal QRS , while the occurrence of tachycardias has separately been found to be largely based on previously identified conditions, such as AV nodal reentry tachycardia, atrial fibrillation, and ventricular tachycardia.


No comments:
Post a Comment